 It’s now been more than three years since I announced I was going to resume antiretroviral treatments. I’ve only posted a handful of updates about my treatment choices since then, and it’s long past time for an update.
It’s now been more than three years since I announced I was going to resume antiretroviral treatments. I’ve only posted a handful of updates about my treatment choices since then, and it’s long past time for an update.
On May 23, 2012, I embarked on my third course of ARVs since 1998. For ten of the sixteen years I have been HIV-positive, I was able to manage well enough without ARVs and I continue to believe there is no reason for otherwise healthy HIV-positive—let alone negative—gay men to take these drugs. To those who want to wave a recent study about the benefits of early intervention in my face, I would ask them why they put so much faith in a science that has utterly failed us to date. The only beneficiaries of the current AIDS drug guidelines are the pharmaceutical companies; the community based organizations they fund and researchers who cannot see past the tunnel vision of their microscopes as they complete more grant funding applications.
Let me tell you what I’ve done to increase my CD4 count and reduce my PCR viral load to undetectable, and then you tell me why we continue to accept their fucking “treatment guidelines” that are over-drugging and overdosing so many gay men.
Reduced dose monotherapy options
My first protocol, which I’ve written about and discussed in a video, was low dose boosted darunavir monotherapy, or LODOBODAMO. Hey, one can not be taken seriously if he can’t come up with clever acronyms, right? Darunavir monotherapy works. It has been validated with mainstream research, primarily in Europe, published in peer-reviewed journals. Why it isn’t more widely prescribed is anyone’s guess, but you can bet the very idea is despised by pharmaceutical executives who would lose a substantial portion of their profit sharing if doctors started routinely prescribing it.
I was excited about the success I was having with reduced dose boosted darunavir monotherapy. My CD4 counts increased to as high as 274 and 13.7%, a significant gain from 70 and 7.6% when I started it, though it did take a year to get there. My viral load dropped to 3 digits, but I’ve never been as concerned about that number and do not consider low-level viremia a major cause of concern.
One other note about what was going on at this time with my medical care at this time. I initiated treatment under the care of an “infectious disease specialist”, aka an HIV specialist. I’ve written about how she prefaced every other statement to me with that holy grail, “the guidelines”. It took weeks to get an appointment and she spent maybe five minutes in the exam room with me. She was pleasant enough, but seemed to put a higher priority on appearing professional, if not officious. She did not communicate with my primary care doctor. Bottom line: we were not a good fit and I sorely needed my previous doctor back in my life.
The family practice doctor I had built such a good rapport with either left, or was removed from the hospital-owned practice she had been at. I was devastated. I had no doctor I could relate to. I finally met with her covering physician, who turned out to be an alright guy. He never argued with me or chastened me. He ordered the labs I requested and wrote scripts if I needed them, but he never really engaged fully in my medical record or my care. In hindsight though, I was fortunate to at least have found a doctor who abided by his Hippocratic oath to “first, do no harm.” I stopped going to the ID specialist and am now determined to never see another one again.
I was also fortunate to have the services of an alternative orthomolecular research clinic that has helped me identify nutritional deficiencies, as well as turned me on to Organic Acid Tests and Comprehensive Stool Analyses, which I consider as essential to understanding what’s going on in my body as any blood test. I cannot emphasize enough the importance of markers found only in human waste that is not considered, or even understood by most allopathic physicians. Despite a gigantic leap in knowledge about the importance of the gut and human microbiome, few doctors consider having their patient’s poo examined for evidence of dysbiosis and other health issues.
Surrogate markers
Back to the numbers. While my CD4 wasn’t as high as I had hoped, I had been on the drugs longer than I originally planned or hoped, and I quit taking them for the third time about a year later. I not only quit the darunavir and ritonavir booster, but for more than five months I stopped going to doctors or ordering labs, due to the disruption I was experiencing with doctors. When I did get labs done, I have to admit I was devastated. The CD4 had plunged to its lowest level ever: 64 and 4%. This was late October 2013.
I went back on the darunavir at full dose (600 mg twice a day, plus 100 mg ritonavir as a booster) before reducing both drugs to a half dose, once daily schedule. By the end of 2013 my CD4 count had rebounded to 180 and my viral load dropped from 450K to 3,320.
I have updated the charts of my various counts and posted them here. Keep in mind that I was still experimenting with interrupted treatment until very recently, and I expect the obvious reversal of CD4 decline to become a steady increase in the future.
On criminality and costs
I continued to take the reduced dose boosted darunavir in 2014, but my stockpile from the previous year (remember, I had taken only half doses in 2013 and then quit taking it, so I had a surplus to draw on) was dwindling the latter half of the year. I knew I was going to have to pay a substantial deductible, regardless of when I resumed buying the drugs, and January wasn’t that far off. I could not afford to pay that deductible in September, and again in January.
I was rescued by an online pal in another country who, like me, had had success with half-dose darunavir monotherapy. He sent me about a three months supply. Despite that, I ended up continuing to cut the dosage of darunavir to 400 mg/day, the dose of the pills I received from Europe. I also ended up paying several hundred dollars for a single month’s supply of the ritonavir booster out-of-pocket.
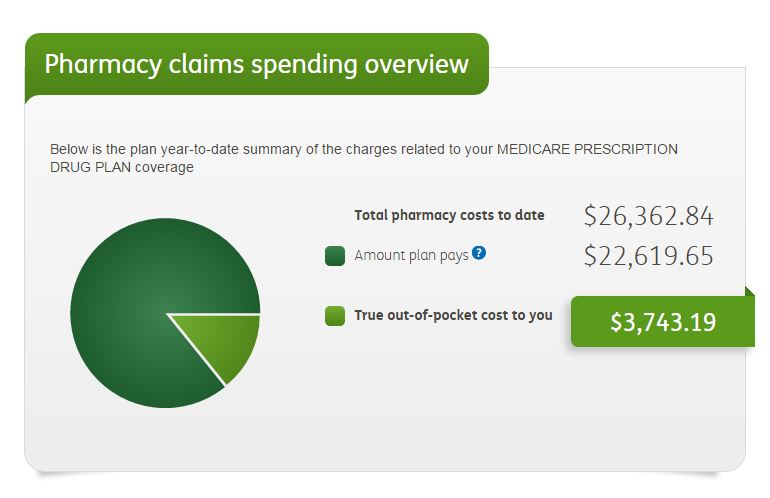
Thankfully, my favorite doctor had returned to private practice by that time and I was once again in good hands. I made a very conscious decision that if I was going to have to pay a few thousand dollars at the beginning of the year, I was going to get the “full monty” of drugs so that once I’d met my deductible and copay, I could hoard any surplus. Call me a crook. Call me a cheat. Call me a drain on the social order. Whatever you do, don’t blame the pharmaceutical companies for pricing the drugs at unreasonable levels that drive people to commit acts of desperation. Dealing with HIV, AIDS and pharmaceutical companies has made me jaded and my conscience does not bother me a bit. The total cost of my drugs so far this year, according to my drug plan, is over $26,000, and it’s only mid-June.
Fortunately, I somehow qualified for a non-governmental assistance program that would cover my out-of-pocket expenses for ARVs in 2015. Probably funded by the pharmaceutical companies. I didn’t ask because I didn’t want to know. I wanted greatest freedom to dabble with these drugs in whatever way suited me. And that’s what I’ve done and am doing.
Darunavir
Although darunavir has a very good safety profile, compared to other PIs, and definitely compared to the NRTI/NNRTI classes of drugs, there was one concern I had about it, and no doubt other protease inhibitors. My stool analyses kept reporting low and declining levels of elastase, an enzyme produced by the pancreas. The labs warned of pancreatic insufficiency, or possibly even pancreatic cancer. I watched as those numbers continued to decline, despite taking pancreatic supplements.
What I learned was that elastase is…. wait for it… a member of the protease class of enzymes. Protease inhibitor. Low levels of an essential protease enzyme. Hmmm. Now, I’ve never claimed to be a rocket scientist, or any other kind of scientist, so the odds of me actually understanding what, if any connection there might be is pretty slim. Still, Google is my friend, so off we go.
Acute pancreatitis is listed as one of the less common side effects of darunavir, and 10% of patients had elevated levels of some pancreatic enzymes…. in the blood. No mention of elastase levels in the stool, though. When the medical informatics company MedsFact asked doctors “Is pancreatitis a side effect of darunavir?”, well over half responded that they “highly suspected” or considered the drug a “possible culprit”.
My doctor assured me that the enzyme levels in my blood were within the normal range. My oncologist said there was no reason to suspect pancreatic cancer at this time. So, what’s going on? I don’t know, but I do intend to try to find out if darunavir is indeed the “culprit”.
I wanted to find an alternative to the protease inhibitor, give myself a break from them and see what effect, if any, that has on my stool elastase levels.
Dolutegravir
In addition to the darunavir, one of the drugs recommended by the Mayo Clinic three years ago was an integrase inhibitor, raltegravir (Isentress), though I had never taken it. However, I had heard from another trusted friend that dolutegravir (Tivicay) had a better safety profile. I also discovered, thanks to Google that doulutegravir was being trialed as monotherapy, and had proven promising at low doses. Raltegravir had failed its trial as monotherapy.
I stopped taking the protease inhibitor and started dolutegravir monotherapy, half-dose, no less, in January. My next labs were two months later and for the first time since April 2003, my viral load was undetectable. My CD4 levels were virtually unchanged, just a tick shy of 200 and 8%. I was emboldened. The whole point of antiretroviral treatment, according to the mainstream is to suppress “viremia”, and I had accomplished that with a very minimal drug regimen. Now I wanted to know “how low can I go”, so I started taking the dolutegravir only five times a week, giving myself and my liver a break on the weekends.
The viral load was detectable the next month, at 34, a number that would have been considered undetectable a few years ago. The next month it was virtually unchanged, at 52. My CD4 counts had risen above 200 and were now at 11%.
I was no longer happy with the low, but detectable viral load. Something in me switched and I now wanted what others were claiming. “Undetectable is the new negative”. Call me a quitter. Excommunicate me from AIDS dissidence. Again. I resumed taking the dolutegravir every day in early May. By June 6 I was undetectable again and my CD4 had risen above 200 (12%) and rising.
That’s where I’m at today. I take a single pill. Not Truvada or Atripla or any of the combination drugs containing NRTI/NNRTIs, the earliest, most problematic and damaging class of ARV drugs. Integrase inhibitors are the newest class of ARVs and I do not doubt for a second that we will discover there is something about them that is damaging to some part of our bodies. That is just the nature of pharmaceutical (and some natural) drugs.
It is my intention to maintain this regimen for the indefinite future. I want to stop fixating on labs, though that seemed necessary as long as I was dabbling with different doses and timing of drugs. My goal is to see my CD4 count and percentage continue to increase, and I expect the viral load to stay undetectable.
I fully recognize the limitations of my trial of one. I do know others are having success with darunavir monotherapy. I don’t know if it is a viable option for most Affecteds with declining CD4 counts, but I suspect it is, and until research dollars are spent validating or invalidating the experience I and others are having with reduced dose or intermittent dosing, we are back to where we were in the 1980s. Like the patients in Dallas Buyers Club, we are on our own. Not only without support from the institutions and funding meant to support us, but sometimes thwarted by them as we seek the best way to care for ourselves with the least risk of harm from drugs that can only be called toxic.
But how am I doing?
I have not yet checked my elastase levels, but hope to get that done before the summer is over. Collecting the samples is not as quick and easy as a blood draw, and right now my life is fairly hectic, in a mostly good way. My energy is good for now, and there is a lot going on in my life that I want to have going on. While that may sound good, it has created new stress for me as well and I was reminded of that just yesterday when I noticed a cold sore forming on my lower lip. That is one of my built-in stress indicators that is hard to ignore.
I am also trying to pass some kidney stones that have lodged in my right ureter. Not fun. And not related to either HIV or the drugs that I’m aware of. I had my first blocked ureter long before AIDS was an issue, let alone ARVs and the resultant medical bankruptcy set me back seven years financially.
My focus for the next few months is on helping my partner sell an investment property; host a visit from my brother and his partner; attend my first ever high school reunion (at which a group of us will host the first-ever LGBT reception); and attend the Midwest Men’s Festival in July. I haven’t yet allocated the time needed to visit my 91-year-old mother this year, and I recently joined a small group of long time gay activists to help commemorate the 50th anniversary next year of the very first national gathering of “homophile” activists, right here in Kansas City in 1966, three years before Stonewall.
Whew! It wears me out just to write it all down. It is also a sign that I am not withering away or rapidly dying from the ARVs as some of the more radical AIDS dissidents insist will happen to anyone who pops a pill in their mouth.
Takeaway
These are some of the key thoughts I have as I write this post and I hope readers will take away from this post:
- There is no incentive for pharmaceutical companies to fund research into ways to decrease the use of ARV drugs. The current AIDS treatment guidelines are created by people with direct or indirect ties to the pharmaceutical industry.
- Thousands of gay men and other patients are needlessly being over drugged and overdosed, because the profit motive is too powerful to challenge the established guidelines.
- There are at least two approved drugs that are good candidates for reduced dose monotherapy: darunavir (Prezista) and dolutegravir (Tivicay).
- We are back to the 1980s. Better treatment choices are not going to come from the government or pharma. Affecteds continue to be at the forefront for identifying and devising better treatment options.






Hi, in relation to your comment about people waving that recent study in your face: At the time of writing this, to the best of my knowledge (and from someone who should know) the study you’re probably referring to hasn’t actually been published yet. What they’ve done is release some of the data that can be made to appear favourable. However, as someone who has read many, many papers about HIV/AIDS, I can tell you that you can NEVER trust only part of the information. You have to have the full paper as published and scrutinise it. What you will tend to find them is inappropriate aggregations that obfuscate potentially contrary information; logical flaws; inexcusable omissions of very important information, the inclusion of which might totally change the meaning of the results; ‘findings’ based on inappropriate assumptions; critical admissions buried in the small text; ‘inferences’ and ‘suggestions’ designed to lead you down a particular line of thinking that the paper does not actually support; data presented in tables that superficially appears to show one thing, whereas reorganising the data shows something completely different; focussing on irrelevant correlations and surrogate markers instead of clinical outcomes; And conclusions which are simply not supported by the data in the paper, among other problems. And sometimes you have to find corresponding papers that contain the other, less favourable half of the information that totally undermines the claims in the first paper. So you’re right to not jump at the claims some may make just yet.
This is very exciting!
If integrate inhibitors like Tivicay are truly only targeting HIV rather than normal functions of the human body, then longterm side effects surely have to be greatly reduced. Do you feel better, even subtly, than you did when you were just taking Darunavir?
Please keep us updated. I am definitely interested in trying Tivicay as a mono therapy.
“Feeling better” is such a subjective concept, but yes… I seem to have better energy, at any rate. There was a problem with looser stools than usual, when I first started the Tivicay, but that seems to have been resolved with a switch in probiotics. Then again, I also started taking liposomal glutathione. And an anti-inflammatory for joint pain. And some Flomax and an herbal prep called stone crusher to try to pass a couple of kidney stones. It’s almost impossible to know when a particular drug and/or supplement is causing an undesirable effect when there are so many changes going on simultaneously.
I want to follow your lead and use monotherapy My doctor told me when I switched to Prezista/Intelence/Norvir that I’d probably be ok with just boosted Prezista but added Intelence for safety sake. That said, I’ve been on this and before that a different two drug regimen for years now with consistently undetectable viral load. Im glad to hear you are doing well. These drugs aren’t all bad.
Found this blog today but I must say I am a bit concerned about several things involving your health. The fact that by your admission you have gown through numerous treatment interruptions is concerning. It carriers significant and well documents risks for viral rebound/drug resistance, acute retroviral syndrome, decreases in clinical markers that are difficult to recover even after the resumption of therapy, progression of AIDS defining illnesses, and and the need for chemoprophylaxis against opportunistic infections as a result of CD4 decline. I am sure these are all issues you have discussed with your primary care physician, but perhaps a second opinion from an Infectious disease doc is a good idea.
The jury is still out on numerous mono-therapies, especially in specific patient types. in your case, I think it might be worth a revisit.
All the best.
Thanks for your concerns. Of course there are risks to any self-directed treatment regimen, just as there are risks to following the official guidelines for ART/HAART. I have never had a AIDS-defining opportunistic infection. Never. I have health issues, as I have since childhood. Intermittent treatment has been found promising for many patients, as has reduced dose and monotherapy. The problem is that this research is not adequately funded and published, imho. Perhaps it may not be an option for everyone, but if half as much was spent studying how to make it a better option, you can bet they’d find ways to tweak it. It is a no-brainer that protocols that reduce the number of pills will never get the attention, let alone support from Pharma, which funds most research into ARVs.
Hi from Europe ! I strongly believe that NRTIs are so toxic (caused me osteoporosis at 26yrs after 10months on Stribild back in 2013) and really can’t understand why so many poz are calling for prep when the side effects on bone and kidneys are so heavy.
I’m actually on a dual drug regimen of Tivicay + Edurant since last week and my doctor has already told me that bc my low baseline VL, once undetectable for few months I can stay on Tivicay monotherapy.
Sascha