
You wake up in your bed and believe whatever you want to believe.
and I show you how deep the rabbit hole goes.”
―Morpheus, to Neo
First off, I generally hate to read anything claiming to be “The Truth”. Such notions just muddy the intellectual waters and sully truth’s reputation. However… that the anti-HIV drug Truvada dares to start its name with the same three letters as truth lends itself so well to some observations I’d like to make that I just couldn’t resist the temptation to make an exception for this headline. If you’re expecting to read the truth here, you’ll likely be disappointed. I don’t know what the truth is. What I’m pretty sure about is that the campaign to convince gay men to take a pill a day to eliminate their risk for AIDS is premised on anything but facts alone.
Today is World AIDS Day, or to use the acronym, WAD, which is still a mouthful, if you ask me. The theme for this year’s event is “Getting to Zero”, the same theme as last year and the same theme as next year. It is surely a marketing team’s wet dream. Zero what? Viral load? New infections? Zero tolerance for stigma, I read on one site. Whatever zero you want to push or pull for, as long as it isn’t $0.
PrEP seems to be on the minds of nearly everyone involved in the response to AIDS, to the exclusion of nearly all other issues. PrEP stands for pre-exposure prophylaxis, which is a prevention strategy that utilizes a combination drug called Truvada, manufactured and marketed by Gilead Sciences, a pharmaceutical company founded in 1987 just to develop antivirals. I can’t help but mention a bit of a disclaimer here. Gilead’s founder is Michael L. Riordan, one of the sons of Hugh Riordan, who founded the Riordan Clinic, which I have attended in Wichita, Kansas and have written about before. Don’t think the irony escapes me. Michael Riordan is no longer an officer or board member at Gilead, which just became the 20th largest corporation in the Standard and Poor 500 about a month ago.
While I don’t intend to write only about PrEP today, it is a lumpy enough construct that it does provide a number of platforms for jumping off onto other issues that gay men just might want to think and talk about.
Truvada better with or than condoms?
Let’s get the hot, sexy stuff out of the way first. Too many gay men are already promoting Truvada as an alternative to condoms for “safer sex”. What’s wrong with this picture? In the first place, there has never been a single study comparing PrEP to condoms. All of the gay men who did take part in the efficacy trials for Truvada were counseled incessantly about the importance of using condoms and following all safe sex guidelines. Remember, these were blinded studies; no one knew whether they were receiving Truvada or a placebo, so there was no incentive for taking risks. Secondly, just a few of the observed side effects of Truvada include:
• mild diarrhea. mild nausea or stomach pain;
• headache, dizziness, depressed mood;
• strange dreams;
• mild itching or skin rash; or
• changes in the shape or location of body fat (especially in your arms, legs, face, neck, breasts, and waist).”
At the risk of being a bit too graphic, just how is being intimate with someone with these symptoms conducive to hotter sex than using a latex sheath?
Condoms can greatly reduce the transmission of other sexually transmitted diseases, like syphilis, gonorrhea and chlamydia. Truvada does not.
A case of 1,000 condoms cost less than $500; while a month’s supply of Truvada costs around $1,200.
HIV, not AIDS
The over-riding message from PrEP promoters is that Truvada reduces risk by factors that are simply not supported by the research to date. Forget numbers like “92% effective”, or “99% effective”. The relative reduction in the iPrex study was only 44%, and the real, absolute reduction, if we trust the calculations of George M Carter, writing for the Foundation for Integrative AIDS Research (FIAR), was much, much less. You can read more about that in my last blog post.
Forget those numbers for a moment and ask yourself: reduction in risk of what? AIDS? No. I have yet to see a single study on PrEP that indicates it reduces the risk of anyone acquiring immune dysfunction and subsequent illness from opportunistic infections. What the studies showed was a modest-to-substantial reduction in the number of study participants seroconverting on a polyreactive test for some proteins assumed to be antibodies specific to HIV, which is assumed to be the sole and sufficient cause of AIDS. If HIV is indeed the culprit, then this is a worthy achievement.
Retroviruses have played a sometimes critical role in our evolution as human beings for millions, perhaps tens of millions of years, and make up eight percent of our genome.
Time will tell if reducing transmission of what may actually be a messenger, or as Peter Duesberg calls it, a passenger virus, will yield a comparable reduction in acquired immune dysfunction in gay men, but I’ll share today some reasons why I doubt it.
History of gay men and viral illness—a perfect storm
“Those who cannot remember the past are condemned to repeat it.” —George Santayana (and perhaps others)
Contrary to the Center for Disease Control’s memo on June 5, 1981, AIDS did not just suddenly appear out of thin air. The first obvious contradiction (deception?) that report states that the five homosexual men with Pneumocystis carinii pneumonia were “previously healthy”. They were not. Gay men, as a group, hadn’t been healthy for at least a decade or two before that report, and statistics supporting that claim have been published in the medical literature many times.
The first front in the perfect storm that led to high rates of infectious diseases in gay men was an increase in the ability to acquire larger numbers of sexual partners, due to social changes. Some will no doubt argue that there has always been homosexual activity among men, as if that disproves the evidence presented shortly. Yes, homosexuals have existed throughout history. What changed, probably shortly after World War II, was a subtle increase in gay visibility. This earlier lack of visibility precluded gay men’s ability to meet large numbers of sexual partners. Bars and other gathering places became more common, at least in larger urban centers, signaling the birth of a new community.
The very sexual liberation that advocates call forth to testify in favor of PrEP began—depending on your sources—either in the 1960s, or perhaps just after, or even during World War II. The defining moment most often cited as the beginning of the modern gay liberation movement was the Stonewall riots in New York City in 1969, though homosexuals had been organizing and protesting before that.
The first stirring of a public homosexual political movement in the U.S. was in the 1950s, with the founding of the Mattachine Society. Discreet bars, just for homosexuals, began opening in the 1960s in numbers significant enough to warrant police attention in the form of raids. The arrival of bathhouses catering to gay men exclusively boomed in the 1970s. The so-called “sexual revolution” was in full swing during the 1960s and 70s, and though straights may have gotten more attention than gays, that was probably due more to public loathing of queers and bulldaggers than the low lighting levels in the tubs.
The baths were also a petri dish for culturing new ways to test the limits of sexuality. First rimming, followed closely by fisting, men’s anuses were—literally—stretched to previously unheard of limits… and at least for some, on a regular basis. Throw in shower shots, and we may have put the final nail in the coffin for our gut-based immune systems.
Narcotic drugs, developed for use in the battlefields of Europe decades earlier, and their variants, found their way into the urban subculture, and gay men who were simultaneously overcoming centuries of oppression and exploring their sexuality by going “where no man has gone before” were frequent users and abusers of these substances. Poppers were ubiquitous at bars and baths. Every gay men who socialized in the 70s inhaled poppers, whether they wanted to or not. There was no way to avoid the fumes in such enclosed environments.
That many of these bars and sex clubs were owned by the same organized crime syndicates that were bringing heroin, cocaine, amphetamines and other immune damaging drugs into the urban cores served as a catalyst for fueling an epidemic of substance abuse in a subset of the gay community.
As if these illicit drugs weren’t bad enough, doctors wore out their prescription pads and pharma-funded pens, dispensing penicillin as both treatment and prophylaxis… an earlier form of “PrEP” practiced 40 years ago, if you will. Something emerged from this storm that had closed in on the gay male community, and today we call that something “AIDS”.
Bacterial
Part of the heritage of gay liberation—sexual freedom, exploration and experimentation—included sexually transmitted diseases. That gay men were far more likely to acquire and spread syphilis and gonorrhea is documented in the medical literature of the time. It is also evidenced by the appearance of public health services that specifically targeted homosexual men. Yes, the first widespread example of social acceptance of homosexuality came from the STD clinics of public health departments in large cities.
Though the emphasis was on the most common and well known bacterial infections, such as syphilis and gonorrhea, which could be successfully identified and treated with antibiotics, intestinal parasites were also starting to get notice. By the time I came out in the mid-1970s, gay men were urged to find gay or gay-friendly doctors to help address our “special needs” regarding medical care. From a article in the Journal of the American Medical Association, dated November 7, 1977:
Homosexual men may be deterred from seeking an examination for sexually transmitted diseases because it would require an open admission of sexual preference. For these diseases to be controlled, gay men must be motivated to be examined for sexually transmitted diseases. If a medical or health professional feels unable to respond to a gay patient’s needs, he should refer the patient to someone who deals well with gay patients. Health care services must be offered in a way that minimizes the anxiety many homosexuals associate with examination and treatment for sexually transmitted diseases.
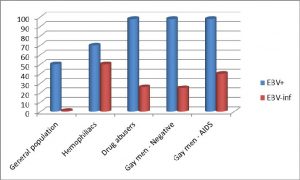
The charts in this post are based on statistics compiled from a variety of sources, mostly from the 1970s and 1980s and were published in Rethinking AIDS (not to be confused with an organization with the same name), by Robert Root-Bernstein. The major “risk groups” for AIDS are identified: hemophiliacs, IV drug users and gay men, both HIV-positive and negative. The column on the left in all charts represents the rate of infection for the general population.


The comparisons are more than striking. They certainly raised my eyes, and they do tell a story about the role infectious disease has played in the history of sexually active gay men.
Parasites
Intestinal parasites and other disruptors of gut health were also being identified during the sexual revolution. In a 1972 letter to the editor of the Journal of the American Medical Association (JAMA), Howard B. Shookhoff, MD, writes:
Such a panoramic succession of single or combined infections is not unusual in the experience of myself and my associates among male homosexuals. Given the multiplicity and versatility of sexual contacts in this group, it is not surprising that fecaloral transmission of a variety of infectious agents occurs frequently.
In 1979, a bulletin of the New York Academy of Medicine begins by stating:
The sexual transmission of enteric pathogens has recently been recognized as a significant health hazard. Sexual transmission of protozoal pathogens such as Giardia lamblia, Entameba histolytica, and Dientamoeba fragilis in the urban homosexual population was first reported in 1972. Since then, several more papers have appeared in the literature describing cases of amebiasis, giardiasis, hepatitis B, salmonellosis, and shigellosis that were sexually transmitted, primarily among homosexual men. These enteric infections, which have traditionally been associated with contaminated food or water and encountered among Americans with a history of foreign travel, are now found in significant numbers among individuals without a history of such travel.
Gay Bowel Syndrome
Gay men were experiencing serious health issues and assaults on their immune systems long before AIDS was identified in 1981, or HIV discovered in 1983. Many gay men met extreme prejudice when dealing with straight doctors, resulting in sub-standard medical care, if indeed they received any care at all. Add this to a burgeoning epidemic of STDs, and one can begin to see how an entire group of increasingly sexually active men were exchanging a lot of different pathogens. For just this reason, when I came out of the closet in the last half of the 1970s, we gay men were being advised to find a gay or gay-friendly doctor. The symptoms I most often presented for involved gastrointestinal distress and diarrhea. When tests for parasites came back negative (these tests are notoriously unreliable), I was either treated presumptively with Flagyl—a very potent antibiotic with serious known adverse effects—or told I might have a sensitivity to dairy!
Meanwhile, in 1976, medical researchers reported:
The clinical and pathological findings in a group of 260 homosexual men comprising 10% of a private proctologic practice are reviewed. A clinical pattern of anorectal and colon diseases encountered with unusual frequency in these homosexual patients is termed the gay bowel syndrome. The clinical diagnoses in decreasing order of frequency include condyloma acuminata, hemorrhoids, nonspecific proctitis, anal fistula, perirectal abscess, anal fissure, amebiasis, benign polyps, viral hepatitis, gonorrhea, syphilis, anorectal trauma and foreign bodies, shigellosis, rectal ulcers and lymphogranuloma venereum.
That is quite a list of complications in the colon and rectum of gay men. To spare the lay reader from having to google all these medical terms, here is a brief (and no doubt incomplete) summary:
- viral warts
- hemorrhoids
- infection of the rectum of unknown cause
- unnatural channels that originate inside the rectum and terminates outside the body, on the buttocks
- bacterial infection of anal glands, resulting in painful abcesses
- tears (rips) in the skin of the anus
- infection of the intestines caused by the parasite Entamoeba histolytica (can become a severe, advanced infection affecting the liver, lungs, brain and other organs)
- non-cancerous growths on the lining of the colon or rectum (can become cancerous)
- viral infection of the liver
- well known, common sexually transmitted diseases
- damage to the anal or rectal linings, such as tears, caused by brute force by a blunt object, such as sex toys, an erect penis, or foreign objects (Coke bottle, anyone?)
- infection with the bacteria Shigella, a common cause of food poisoning in other people
- sores in the rectum
- chronic (long-term) infection of the lymphatic system caused by three different types of the bacterium Chlamydia trachomatis
Since this list is from research published in 1976, it is probably representative of a good portion of the height of the so-called “sexual revolution”. The significance of this “syndrome” (sound familiar?) may be far greater than any of us realized in 1981, when the first cases of modern day “AIDS” were announced by the CDC. Since then there has been a great deal of research into the role of the gut in human immune health. While it is merely speculation on my part, it does not seem unreasonable to suspect that anything that damages the GI tract is likely to impact the immune system.
Enter the viruses
Though not as easily identified forty or fifty years ago, there is little doubt that other viruses were also a part of the pathogenic milieu in sexually active gay and bisexual men. From the same source as above, from data gathered in the 1970s to late 1980s, a similarly high rate of multiple viral infections is seen in gay men, and even more so for those who later test positive for HIV antibodies. The charts below represent the rate of exposure (blue) and active infections (red) of cytomegalovirus (CMV), Epstein-Barr virus (EBV) and Hepatitis B virus (HBV) in the general population, vs the rates in the high risk groups for AIDS: hemophiliacs, intravenous drug users and gay men.


Talk about denial
It is hard for me, as a gay man and a gay activist since the 1970s, to understand why my community is still in denial about what these measures represent. There is nothing sex-positive about having a similar prevalence of disease as groups that depend on intravenous blood products for their lives, or those who are victims of drug addiction.
I can hear the howls of protest now. I must be an old, bitter self-hating homosexual to even dare to raise this question. That would be the easy cop-out. I urge gay men reading this to do their own research, and then some self reflection about what kind of community we want to have in the future. I am old, at least in gay years. I no longer have sex with other people. It is easier for me to accept that we need to make some changes than it will be for a 20- or 30-something year old virile and attractive gay man. That does not, however, change these facts.
I’m not blaming gay men, nor trying to “slut shame”, so spare me the epithets. Like the popular status coined by Facebook: “it’s complicated”. It was not our fault that doctors and the medical establishment, along with the rest of society, turned their backs on us during most of the last century.
It is not our fault that our history was heavily influenced by external and internalized messages that something was wrong with us; that we were inherently diseased and perverted.
It is not even our fault that our track of the so-called “sexual revolution” of the 1960s and 70s took an exponential leap beyond that of heterosexuals.
I am talking about some very sexually active gay and bisexual men. I am not talking about lesbians. There is a biological factor at play here as well. Google it. Men’s sex drives are just wired differently than women. We are more ready to have sex at any moment and more often. There are few aspects of the AIDS epidemic more telling than the astounding difference in prevalence of HIV and AIDS in gay men vs. lesbian women.
Our history of “liberation” is entwined with some rather unsavory partners. One of the first opportunities for gay men to meet each other were the bars, which were not yet acceptable, or perhaps even legal businesses. They were often owned and operated by organized crime figures. They were never intended to foster “community”, but to make a profit… clients be damned. In addition to high rates of STDs, gay men also hold the honor of having one of the highest rates of alcoholism and tobacco addiction, all promoted and marketed to us in the name of greed.
Gay bars were not the only focus of the mob, of course. Indeed, they were something of a side business for them. Organized crime syndicates and gangs had long been the primary source of narcotic street drugs and prostitution. It takes little imagination to see how these influences were marketed to an already captive audience. Add high rates of illicit drug use and addiction to the mix of cofactors likely to damage the health and immune systems of gay men.
It would be so easy to suggest that this was just the case 50 years ago, but there is evidence that the LGBT community has not yet shaken off the dubious honor of having higher rates of addiction, and that addiction contributes to poor health and strains our immune systems.
Poppers and drugs
We can’t just blame the mob, though. Greed and ambition rules most “successful” business men, and nowhere is this more true than in the use of nitrate inhalants, also known as “poppers” among gay men. The damage poppers can cause is indisputable, though the question of whether some of the diseases that define AIDS may be caused by them—especially Kaposi Sarcoma—does not need to be addressed here. Only a fool would argue that inhaling the stuff is harmless, so for now I’m willing to simply add it to the list of multifactoral possibilities unique to gay men that can make us ill, or damage our immune systems.
Multifactoral
There. Why did it take me so long to get around to using this word? I think what troubles me most is how and why we gay men embraced the viral causation theory of AIDS so quickly and now defend it so vigorously. It changes things from “it’s complicated” to “it’s simple,” and that’s a very attractive option. Unfortunately the evidence does not really support the notion as well as it does other explanations for the cause of AIDS.
Robert Root-Bernstein, the author of the book I derived the above charts from, presents a number of alternative hypotheses for AIDS, other than a single pathogen causation. One that makes so much sense it’s hard to ignore has been…. well, ignored. What effect does repeated exposure to so many multiple pathogens—to say nothing of cofactors, such as substance abuse, alcoholism and tobacco use, among other things—do to a person’s immune system? How many battles can one’s immune system mount against potentially life-threatening viruses before it tires and some components, such as t-cells perhaps, erode? What is the likelihood that having multiple viruses in a single host won’t combine and create some synergistic effect or action that might appear to be “new”.
It is so logical that it seems obvious. Retroviruses are an innate part of the human genome. They are not known for being harmful or pathogenic. That HIV exists, I have no doubt, but I strongly suspect it is more likely a marker than the cause. Fighting HIV may well be an exercise in futility, but I’ll get back to that in a moment.
First, allow me to share a couple of anecdotal stories to introduce you to a couple of friends who have recently had a strong influence on me. They don’t prove anything, but they may help some of you understand better why I remain on the side of skepticism about the role of HIV in the cause of AIDS.
Tony
No, I won’t use his real name, because he is still alive and is still my friend, but to this day I cannot get this part of his life story out of my head. I’ve known Tony for decades. He spent a number of years working at a popular gay club in one of those meccas the rest of us gay men periodically escape to. Doesn’t matter whether it was Provincetown, Fire Island or Key West. He was damned good-looking and as a bartender, had his pick of tricks for any given night. His sexual acquisitions were legion, and different men from around the world strolled through his door every night for the better part of a decade.
Tony finally decided to face his alcoholism and addictions and entered recovery about a decade ago, but he was never able to overcome the sense that something was wrong because despite being one of those “fast track” gay men, he continued to test negative on the HIV antibody tests. He even enrolled in a study designed just for such men. Did he have some sort of special immunity to HIV? Or was there something about the fact that he was a 100% exclusive “top”?
A few years ago, I got a call from a mutual friend. Tony was in the hospital and needed help. He had been treated for pneumonia and then, a week or so later, was back in the hospital, this time with pleural effusion. Whatever had caused his infection was now between the lining of his ribs and his lungs, filling the pleural cavity with pus. They punctured his chest two separate times, between the ribs, and inserted tubes to draw off liters of this goo.
I packed my bags and went to help him recover at home. We tried to get detailed medical records, but for some reason he never got copies of them for himself. Because Tony was gay, and not an old man (he is several years younger than me), the doctors at the hospital immediately suspected an HIV-related opportunistic infection, probably pneumocystis jiroveci (previous carinii). Tony told them his story, and asked them to test him again. The result was negative, so they continued to treat for typical pneumonia, rather than put him on antiretrovirals, as they would if he were HIV-positive. The conventional treatment worked.
Now, I cannot analyze Tony’s case as definitively as I would like, because I do not have access to his medical records, and because having too much information is not as important to him as it apparently is to me. Still, his case begs the question: why are we not looking more closely at people like him, who meet all criteria for risk of immune dysfunction, just because they happen to test negative on a polyreactive antibody test?
Why is the medical research establishment not more interested in the state of Tony’s immune system? Neither Tony nor I know what his t-cell counts are, for example. Because he is antibody-negative, it is unlikely that anyone ordered a PCR viral load test (though I can’t say with certainty that they did not). Did Tony have exposure to any, most or all of the STDs and viruses mentioned above?
Tony’s case doesn’t “prove” anything in particular, other than sometimes gay men get sick with a life-threatening case of pneumonia that just happens to look exactly like those that occur in people with AIDS, even though their antibody tests are negative.
David
I will use David Ray Stanturf’s real name. David died September 17, 2010, just three days shy of a year after I had reconnected with him after a long separation. David was a good friend of mine in the 1980s and early 90s. He volunteered during my campaign for city council in 1991, but we had a falling out shortly after that. David was the founder of a new gay publication while I was the Kansas City editor for the News-Telegraph, a real and serious gay newspaper, as opposed to the so-called “bar rags” in town.
I don’t remember when we tricked, and I guess it doesn’t really matter. It was one of those casual things that happened between friends. No big deal. A pleasant night together, as I recall, but not significant enough to ever evolve into an affair. I’m pretty sure we both followed the rules about being “safe”, especially knowing what I know now. For what it’s worth, this was nearly a decade before I tested positive myself.
After losing track of each other in the mid-1990s, I ran into David and his boyfriend at the screening of the AIDS dissident documentary House of Numbers in 2009. I discovered that he had followed this blog for awhile and that is how he had learned about the film. A group of us went out to eat after the show, and my friendship with David was quickly renewed.
It took a few years, but David finally opened up to me with his own story. One of my biggest regrets will be that I didn’t document it better, but David’s demise happened too suddenly. I have never shared this before, and have thought about it for some time, but based on the earnest discussions David and I had the last year of his life, I’m certain he will not object to me telling it now.
David tested positive while in the military, or perhaps as he attempted to enlist. I do not know what year this happened, but I remember it was very early in the epidemic. It had to be after the Gallo test was approved and the military had started testing, which was 1985. David was born in 1966, so it was probably within a few years of then. At that time, a positive test was a death sentence, and David was devastated. For some reason I no longer recall, he chose not to take any drugs. I suspect it was because many of us thought AZT (the only drug available) was more poison than medicine.
Then a strange thing happened when the PCR viral load test became available in the mid 1990s. Despite being positive for several years, perhaps even a decade, and despite never taking ARVs, David’s PCR test was “undetectable”. No wonder David was a skeptic. Despite having no evidence of virus in his blood, David told me he was often urged by doctors to take ARV drugs.
Not that David did not have some serious health issues. He was positive for the Hepatitis C virus, and though he had learned to be skeptical about such tests, it was obvious that his liver was in distress, and failing. I could not help but empathize with the dilemma David faced. The medical system had earned his distrust, yet he could not deny the swelling in his belly, or the increasingly jaundiced look of his face. He was admitted to the the University of Kansas Medical Center and started receiving liver dialysis, but doctors told David that he could not survive on that treatment. He needed a liver transplant.
A couple of problems with that, though. First of all, there was a waiting list for all potential recipients, and not everyone would survive the wait. Secondly, and more frustrating for David, was that the doctors told him he would never even make the waiting list as long as he refused treatment for HIV. “Where’s the HIV?” David asked them, but they could not or would not answer.
What does all this have to do with PrEP?
These stories are just two examples of many in my life where the dominant HIV causation theory just doesn’t make sense. Truvada is for HIV, not AIDS. Remember when we knew the difference between the two? When exactly did that change?
I know of no way to give more than a small part of our community’s history necessary to make the case for my objection to the current all-out promotion of Truvada-as-PrEP to gay men. Go back to the beginning of this post: we cannot make sound choices that affect our future without understanding and learning from our history… our past.
Gay and AIDS activists have hammered out a message of “safer sex”, based primarily on consistent condom use, for nearly three decades. Is it working or not? If so, why do we need to roll out prohibitively expensive PrEP to fill Gilead’s coffers? If not, how do we reconcile the knowledge that PrEP has never been studied or tested as a substitute for them?
I’m willing to grant that gay men are entitled to use PrEP… provided they have access to all the information they need to make an informed decision. Informed consent has been a hallmark of the HIV and AIDS research and prevention efforts for three decades, and that shouldn’t be waived for the campaign favoring PrEP.
Gay men deserve to know that all the claims for Truvada reducing the risk of acquiring HIV-positivity are based on trials—funded by Gilead—that emphasized the importance of using condoms and following all other possible measures of safer sex guidelines, as I wrote at the beginning of this post.
If one does choose to take Truvada to cut their risk, the rate of reduction is not 99%. That is a theoretical number. In the studies, the rate of reduction was 44%, which ain’t bad, so why milk the numbers?
Regardless of which number you choose to believe, know that they refer to relative risk. I’ll let Connor explain that the absolute risk is a much different number:
So there were 100 infections over a median of 1.2 years on the drugs: 36 in the drug arm and 64 in the placebo arm. The 44% we hear about is the difference of 100-36/64 or 44%. But another way to look at it is the ABSOLUTE RISK. That is, 36 out of 1251 people in the drug arm became HIV+ over a median of 1.2 years. The calculation of 36/1251 yields about 2.87% risk of becoming infected on the drugs, but that is a rough estimate. On placebo, 64/1248 would be 5.1% or an absolute risk reduction of 2.2%/year. According to lead author, Robert Grant: The annual incidence was 3.86 in the placebo group and 2.16 in the FTC/TDF group.
In other words, more than half as many men taking Truvada still got HIV as those taking the placebo. Connor goes on to make it even simpler, for those of us who didn’t study statistical analysis:
Look at it this way. Say you are an HIV-negative gay man. You ask your doctor to prescribe Truvada. She agrees. You must then take it every single day. You must be able to pay for it. You must be able to tolerate the unintended weight loss and nausea that a significant number of participants experienced (see FN2). You must face the risks of bone destruction over time and the slight risk of lactic acidosis. You must use condoms still. And after a year, your chance of becoming HIV infected will have been lessened by 1.7% than had you not taken the drug and done all those things we know can drastically reduce the risk of infection.
So much for the myth of 99%.
There is other information that one must consider before taking Truvada as PrEP.
There is no clinical evidence that Truvada will impact the disproportionately high rates of other viral, bacterial, fungal and mycobacterial infectious diseases found in gay men. If we discover that Root-Bernstein and others are correct; that the causes of AIDS are multifactoral, or if it is determined at some point that “HIV” is actually a messenger, or even passenger, and not the cause of chronic immune dysfunction leading to opportunistic infections, we will have lost even more decades in getting the upper hand over the real cause(s) of illness in our community.
No one knows what all the long-term effects of Truvada will be, though we can be certain there are some. We’re already statistically sicker than most other groups of people, and now we are going to spend a fortune for the opportunity to see increased rates of liver disease and other evidence of long-term toxicity in our community’s future? How does this strategy advance our sexual liberation and claims for equality?
Let me be clear and state it again: I am not trying to argue that PrEP should never be considered as an option under any circumstance. I’ve discussed this with some friends who make a case that they have truly weighed the risk/benefit ratio and have made their decision. They have only my support.
As I stated before, the problem is the increasing drum beat that all sexually active gay men should be on Truvada as part of some campaign to wipe out AIDS. That’s not what the research shows and it’s another example of gay men being deceived by a marketing campaign that is being financed by corporations that stand to profit from us making “the right decision”, that is, the decision that’s “right” for Gilead.
What I object to is the subliminal message that is creeping into this campaign by self-described “Truvada Whores” that if you take Truvada you can ditch the condom.
What I object to is the lack of a loud and public outcry against Gilead for holding all of us—gay and straight alike—hostage for the exorbitant price; a price that is increasingly being picked up by insurance companies or government assistance programs that only ratchet up the cost of health care for all, while Gilead makes millions in profits.
What I object to is the apparent satisfaction of too many gay men that Truvada is “good enough” as an answer to the devastatingly high levels of disease in our community. We are still looking for the answer in a pill, and not working our asses off to reduce the rate of all infectious diseases in our community.
So, we’ve now got PrEP. It’s not enough, and we’ve spent enough time celebrating it and World AIDS Day. It’s time to demand more.
It’s time we demand more from the enormous research system that has been built upon the single pathogen causation theory and to this day has no cure or vaccine in sight.
It’s time we demand more from the expensive social care industry that has been created, employing thousands of high payed workers.
It’s time we held activists who once protested Pharma greed accountable for shifting their allegiance to promoting Gilead’s latest illusion of “safety”.
It’s time we demand more from our community leaders. We’ve founded organizations that raise and spend hundreds of millions of dollars on treatment, care and prevention, and we get…. what? A blue pill?!
And yes, it’s time we demand more from ourselves. It is complicated, but it can be understood. There is no simple answer that explains why the immune systems of many gay men are as likely fail as those of hemophiliacs, IV drug users and those who live in poverty, with little or no clean water or even basic medical care.
All I need to know, I learned from Wanda Lust.
A drag queen named Wanda Lust used to tour the gay bars and bathhouses in a van sponsored by the Kansas City, Missouri Health Department in the late 1970s to perform testing for syphilis and gonorrhea. The importance of Stephen L Jones’ life was his commitment to service within the gay communities of Kansas City and Chicago in the 1970s, but there’s another reason I’ll never forget “Nurse Lust”.
That the health department of a mid-sized, Midwestern city like KC was devoting so much of their limited public health resources to the sexual health needs of gay men in 1978 should not be overlooked as one of the clues about what led to “AIDS”. Gay men were dealing with multiple infections, including viral infections like herpes, cytomegalovirus, Epstein-Barr virus and more.
There never was a need for a new virus to explain why our immune systems eventually gave out. That rabbit got pulled out of the hat of Dr. Robert Gallo, who has been exposed as a huckster; a fraud and a thief.
At the time Nurse Wanda Lust was doing her tour of duty, doctors were proactively prescribing a pill to healthy—i.e. non-infected—gay men to protect us from these STDs. It was called penicillin. That practice soon proved disastrous, as the pathogens we were trying to avoid developed resistance instead, making them even harder to resolve, and perhaps… who knows… contributed to the evolution of AIDS.
Internalized homophobia and sex-negative messages
Lest anyone accuses me of suffering from internalized homophobia (though, I surely do as much as every other gay man who grew up in this culture), ask yourself how much self-hatred does it take to turn an eye on the evidence presented above? For that is the choice: state it and face it, or pretend it doesn’t exist.
The usual responses to arguments such as the one I’ve just tried to make is that it is sex-negative, and that gay men will be gay men, and since they won’t change their behavior, PrEP is better than nothing.
The claim that any call to learn from our history, witness our current state of affairs and ask what we want to model as a gay male community in the next generation and beyond is “sex-negative” is a misguided reaction. Hell, it’s a red herring. I don’t want men to stop making love or enjoying their sexuality. What I am suggesting is that we look beyond the pill to ways to create and embrace a way of being sexual that doesn’t put us at risk of illness. Few things are less sexy than an emaciated body, or diarrhea, for chrissake.
What I am proposing is that gay men continue to explore and learn new ways to make love and share intimacy, and not spend thousands of bucks just so they can fuck bareback.
The suggestion that gay men can’t or won’t change behavior is nonsense. Remember when we could smoke on airplanes? Or when we could drive without wearing seat belts? When it was perfectly acceptable to throw trash out the car window? There are many examples of public campaigns that have changed people’s behavior. Instead of saying it can’t be done, let’s talk about what the first baby step might be.
I’m more proud to be a gay man today than I have ever been in my life. I am in awe at the things my community has accomplished, and I look forward to seeing even more objectives met, and new goals set. In fact, I’d like to propose a new, ambitious goal for my community. How about becoming one of the healthiest subsets of human beings? How about reducing the rates of addiction and compulsive behavior? And how about we do that without sacrificing our freedom to express ourselves sexually in ways that nurture and strengthen us as people and a community?
How about we start by planting a seed that proclaims the best sex possible between men are acts of intimacy where all partners involved know each others’ name?
How hard can that be?






{kind=link}
{kind=link}
Well done… I am one in the gay minority that has always held a certain amount of distance around using Truvada. Mostly my reasoning has been that we seldom know what long terms there will be with any drug since they are introduced before studies of 10 years or longer are made–especially for a drug one takes daily. Second of all, the drug companies now have the entire LGBT community in their pockets. You have people with HIV positive people on cocktails,HIV negative people on Truvada, and transgender people on a life time use of steroids. Bingo. And, it becomes a social/political issue when only the wealthy can afford these drugs.
You included a lot of false statements here. I do think you make some good points, but you need to do your research better. It’s 2015, now there’s more info. Come one, update this article.
Thanks for reading and commenting, but you don’t offer a single specific example of a “false statement” for me to respond to.
Jonathan,
This is Bob Root-Bernstein. Keep up the well-informed arguments! And hold fast to your position. There will be a couple of papers appearing later this year that will demonstrate beyond doubt that HIV requires cofactors to enhance its acquisition and to speed its progress to AIDS. These papers are by a major HIV researcher who finally realized that HIV by itself can’t explain the epidemiology or pathogenesis of AIDS (i.e., why some people who are exposed don’t get infected and why the people in Africa have such a different rate of susceptibility to people in developed nations). So this guy decided to look at other factors that might influence the spread of AIDS and, lo and behold, he found them in spades. As you say, we’ll have to face up to the facts now… and the sad fact that so much was ignored by so many for so long….
Thank you, Dr. Root-Bernstein! I look forward to further communication with you.
So..did the paper(s) come out?
I don’t know. I need to follow up with Robert. I need to do a lot of things, but am having trouble finding the time to do them.
One year on and Root-Bernstein hasn’t followed up. Co-factors were identified as long ago as the late 80s by leading proponents of the ‘HIV’ theory, so that’s nothing new based on a belief that the raised proteins seen in a ‘+’ ‘HIV’ test were a marker and nothing more. Also until the CDC stopped monitoring them, there were 1000s of people ill and dead from so-called ‘AIDS’ defining illnesses who never tested ‘+’ for ‘HIV’. And where are the seriously ill and dying in ER rooms among the 70% of officially diagnosed ‘HIV+’ people in the USA (45% on average in Europe) who are NOT on compliant ARV treatment? None to speak of.
I think it’s kinda’ harsh to accuse Root-Bernstein of “not following up.” Publishing in peer reviewed journals can be time consuming and very difficult. Especially if one is bucking the conventional wisdom that their peers have swallowed hook, line and sinker.