
During our last office visit a couple of months ago, the infectious disease specialist I am now seeing repeatedly referred to “The Guidelines”, as if they were some kind of Holy Grail for treating her patients. The guidelines she was referring to are actually several documents, published by the U.S. Department of Health and Human Services (HHS), that tell doctors when and how to treat HIV-positive patients with pharmaceutical antiretroviral drugs (ARVs).
Despite being published and sanctioned by a government agency, The Guidelines are actually established by a 38-member panel of “experts”, more than half of whom acknowledge direct financial ties to pharmaceutical companies. A quick Google search reveals that at least some, and perhaps most of those reporting “none” on their financial disclosure are employed by governmental agencies, universities or major medical centers with close financial ties to Pharma. Since the link to these disclosures on the NIH website is broken as I write this, making the financial disclosure pages hard to find, I’ve taken the liberty of posting them here.
The latest guidelines for adults and adolescents were updated March 27, 2012, and the biggest change made was to recommend ARVs for everyone who tests HIV-positive, regardless of CD4 count, or general health, despite the fact that many HIV-positive people remain healthy for years, decades, and possibly their entire lives. This harkens back to an earlier era, when the first protease inhibitor drugs were coming to market, reversing late stage illnesses in some severely ill patients and resulting in a new AIDSpeak term, the “Lazarus Effect“. It is a replay of at least two earlier versions of “hit hard, hit early“, and there’s no reason to believe it will not ultimately be seen as a mistake, as was the case in its earlier incarnations.
The most obvious problem with the concept, is the difficulty of trying to manage long-term toxicity and adverse effects from the drugs. Pharmaceutical companies have made some changes, such as reducing dosages, and downgrading the roles of the harshest of the drugs, while continuing to insist that combination therapy is necessary to avoid resistance. That this repacking of old products as new options also happen to extend patent rights, and therefore profits, is not incidental.
Long term adverse effects cannot be determined in 48-week clinical trials, and lowering doses does help reduce the most obvious signs of toxicity. What has not yet been closely studied are the cumulative effects of long-term (read: lifetime) use of combination drug “cocktails”, but it doesn’t take a genius to figure out that they are bound to occur, as the AIDS drug guidelines are now promoting AIDS drugs even to sexually active, young gay men as prophylaxis. How can such a policy co-exist with the notion that the HI-virus is susceptible to resistance and mutations when confronted with these drugs?
Consider also that healthy people are far more capable of metabolizing the drugs for a longer period of time and with fewer obvious adverse effects, than someone who is already sick, or has been repeatedly ill, or exposed to pathogens and treated with multiple courses of antibiotics and other drugs, as was the case with early AIDS patients. The inevitable alarming studies and reports on long-term adverse effects and toxicity can thus be delayed and diluted by introducing this healthy cohort into the puzzle.
There are other guidelines for pregnant women, children, and older Affecteds, as well as guidelines from organizations like the World Health Organization and The International Antiviral Society–USA (IAS-USA). Regardless of the official source, nearly all of the data supporting these official pronouncements are from research conducted by the manufacturers of the ARVs.
The Panel’s recommendations are primarily based on clinical trial data published in peer-reviewed journals and data prepared by manufacturers for Food and Drug Administration (FDA) review.
Like so much of AIDS research, treatment guidelines must be considered with a skeptic’s eye. It is important to be mindful, for example, that the trials used to arrive at these recommendations do not include information about actual progression to disease or death, but are solely concerned with controversial surrogate markers, primarily PCR RNA, or so-called “viral load”.
Few of these trials include clinical endpoints, such as development of AIDS-defining illness or death. Thus, assessment of regimen efficacy and potency is primarily based on surrogate marker endpoints (HIV RNA and CD4 responses).
The dilemma: What do ARVs really do?
Before I go any further, I want to reiterate that this admission by HHS that all understanding about treating AIDS with ARVs is based solely on surrogate lab markers, rather than actual health, based on clinical endpoints, is disconcerting, to say the least. Much of what passes for “health care” in the U.S. relies on studies conducted by pharmaceutical companies—an industry that spends $19 on marketing and promotion for every $1 it spends on research.1 Making numbers move on lab reports is no guarantee of improved health, and that is true of conditions other than just “HIV disease”. Rates of diabetes, hypertension and hypercholesterolemia have all been manipulated simply by moving the goal posts, i.e. changing the definitional ranges of surrogate markers.2, 3, 4
Having said that, I’m not willing to throw all surrogate markers out of the window, either, and I haven’t changed my opinion that long term declines resulting in extremely low CD4 counts is likely an indicator of immune collapse that Affecteds dare not ignore.
When faced with poor health and changes in these surrogate markers, it is not unreasonable to consider them, as pieces of a much larger puzzle. And that brings us back to the point of this particular post.
There is a potentially promising treatment option for those Affecteds who find themselves facing the difficult decision about whether or not to start—or restart—antiretroviral drugs. It’s called low-dose monotherapy—the use of reduced doses of a single class of ARV—and it is strongly discouraged, at least in the United States, despite evidence that it works.
Darunavir
The primary drug used in the treatment strategy I am referring to is called darunavir, also known by its trade name, Prezista. Darunavir belongs to the class of ARVs known as protease inhibitors (PIs), the so-called miracle drugs that were heralded as “life-saving” when they debuted in the 1990s, provided they were used in combination with drugs from other classes, such as nucleoside reverse transcriptase inhibitors (NRTIs ), non-nucleoside reverse transcriptase inhibitors (NNRTIs ), and more recently, entry inhibitors and integrase inhibitors.
The development of darunavir has an interesting history. It was named after Dr. Aruna, the discoverer of the key molecule, which is a naturally occurring protease inhibitor found in fungi. The primary focus of the development of darunavir was to avoid some of the problems with first-generation PIs: resistance, and adverse effects. Clinical trials have demonstrated success on both counts.
For someone like myself, who is striving to embrace natural healing whenever possible, it’s also good to know about darunavir’s basis in nature. When I talked to Marco Ruggiero last year, he told me, “darunavir is the closest to a natural product that you can think of, because it has been designed, bearing in mind, how natural protease inhibitors work… with less side effects than other antiretroviral drugs.” Ruggiero has been researching PIs for non-AIDS related issues since the 1980s.
Multi-drug cocktails and drug classes
When AZT monotherapy failed to halt AIDS in the 1980s, pharma giant Burroughs Wellcome pulled out the stops to prevent anyone from blaming the drug, despite its reputation as a known “fail” for cancer, as well as extreme toxicity. For a few years, new drugs followed in AZT’s footsteps, claiming to interrupt the viral life cycle at the point of reproduction called “reverse transcriptase”. There are two (or three, depending on how one counts) classes of these AIDS drugs: Nucleoside/nucleotide Reverse Transcriptase Inhibitors (NRTIs) and Non-Nucleoside Reverse Transcription Inhibitor (NNRTI).
Some critics of these drugs in the AIDS dissident community denounce them as “DNA chain terminators“, claiming that they not only stop the HI-virus from replicating, but also interfere with DNA replication in all cellular mechanisms, making the drugs cytotoxic. Others go to great length to disagree on that point, but instead allege that drugs like AZT cause mitochondrial damage. Regardless, it’s a safe bet that these drug classes are among the highest risk for patients, in terms of adverse effects and long-term toxicity.
It has become Gospel for AIDS drug specialists prescribing Highly Active antiretroviral Therapy (HAART), more recently referred to as combined antiretroviral Therapy (cART), to start with at least two NRTIs. Indeed, the pharmaceutical companies have encouraged this practice by re-packaging older drugs into combination tablets, thus resetting the clock on their patents, and keeping prices and profits high, with minimal investment in research.
While a typical “AIDS cocktail” contains at least three drugs from two different classes, the reality is that many Affecteds are taking combinations of as many as five or six or even more different drugs.
The new monotherapy
The term monotherapy, in this context, refers to the use of a single class of ARV drugs. Darunavir has become the preferred drug of choice for this new vision of monotherapy for many of the reasons I’ve already given, and it has been so successful at changing the orthodox AIDS surrogate markers of CD4 and PCR RNA viral load, that some researchers, primarily in Europe, have broken rank with the mainstream ARV multi-drug “cocktail” mindset and decided to see how well patients might fare on monotherapy. I first heard about monotherapy more than a year ago, mostly from friends in Germany and Italy, where the ARV mindset is not yet as rigid as it is here in the U.S.
The term “boosted” acknowledges the use of a second drug, at low dosages. Retonavir (Norvir) is also technically a PI-class drug, but its real purpose is to increase the availability of darunavir by interfering with the metabolism of that drug, which allows for lower dosing. At least that’s the idea. I’ve heard some reports of successful monotherapy, even without the Norvir “boost”, but have seen no research results yet.
Today, there are so many references to research and trials on boosted darunavir monotherapy (BDM) that I don’t know where to start with citations. A simple Google search will be revealing for anyone who wants to verify for themselves just how promising the research is. There is a fairly good basic overview of the two main studies that have been going on for more than three years now here. Since that report was written, these trials continue to garner favorable reports regarding efficacy, reduced adverse effects and reduced cost.
Despite complaining that data from clinical practice is lacking, this recent meta-analysis, published less than three months ago in Journal of the International AIDS Society, seems to not be focusing on whether boosted PI monotherapy is as good as multi-class cocktails, but rather which PI is better: darunavir or lopinavir (spoiler alert: darunavir wins).
There are some caveats to all these positive research reviews. The studies that I have seen all required participants to already be on “successful” ARV treatment, usually defined as having a sustained VL <50. In other words, people like me, who had not been on ARVs for 10 years, had a viral load of >1M and CD4 count of 70 were not included.
When resistance is futile
One of the biggest boogeymen used to try to scare patients and doctors alike into “compliance” with The Guidelines for antiretroviral drug treatments is the risk of so-called “resistance”, which is another term used to explain “treatment failure”. Both are loaded terms that have been built on a sandy beach somewhere in PharmaLand, and I’m not going to go into detail about them here. Suffice it to say that the assertion is that any monotherapy is likely to result in resistance to some ARVs. My question is: How can a patient develop resistance to a drug or class of drugs that they are not even taking? This is one more gap, and imo gaff, in the AIDS drug establishment’s house of cards.
There are a few reasons why drug resistance should not be a significant factor in considering BDM. First of all, darunavir was specifically designed to resist the tests used to determine resistance, if that makes sense. Secondly, there have been almost no reports of resistance to darunavir in the clinical trials to date, at least not in the monotherapy arms. Resistance to NRTIs, on the other hand, continues to be reported in the combination drug arms.
Where angels fear to tread
Needless to say, I obviously have some issues with the authoritarian nature of “HIV medicine”, and given my low tolerance for ARVs in the past, I was not looking forward to re-starting them, and was especially anxious about having to deal with the system that controls them. Once I had decided that resuming ARVs for awhile was probably in my best interest last year, I got much more serious about investigating options, and BDM quickly became one of the most attractive possibilities.
My CD4 count dropped below 200 for the third time in my life on March 12, 2012. My family practice doctor, who has been supportive of my decision to resist taking ARVs as long as possible, offered to refer me to the renowned Mayo Clinic in Rochester, Minnesota for a consultation on March 29, once I told her that I was reconsidering the drugs. Looking back, I notice that I have never blogged about that trip, though I did post some observations on my Facebook page.” Going to Mayo is kinda’ like going to Disneyland,” I told my doctor. “Everyone should probably do it at least once, if just to be awed, but I’m not interested in going back.”
Here are the ARV cocktail recommendations I was given by the HIV experts at Mayo:

For those who may not be fluent in all of the names for AIDS drugs, zidovudine is AZT, the first, and one of the most controversial and notorious prescription drugs to be approved by the FDA for AIDS. Needless to say, my jaw dropped. I was shocked. I have had to listen to AIDS apologists dismissing dissidents for “harping” about AZT, claiming that it is no longer prescribed, which is blatantly untrue, and they know it. After hearing over and over and over again how much AIDS drugs have been improved, I went to one of the premier medical institutions in the United States where I was presented with a menu of recommended drug cocktails containing three NRTIs—including AZT—all approved 20 or more years ago, plus raltegravir (Isentress), a drug from one of only two truly “new” classes of drugs, an integrase inhibitor approved more than 5 years ago.
OK, folks. Reality check here. I am NOT going to take those drugs. No way. Period. Nada. Nope. And, by the way… what the hell are you thinking of, considering you know my story? After some foot-shuffling, it turns out that the above combos were the only ones they could recommend under The Guidelines that did not interact with some of my herbal and nutritional supplements!
<sigh>
“Which supplements,” I asked. “Did it ever occur to any of you (there were now three doctors and a pharmacist in the small exam room with me) to ask me how wedded I am to my supplements, before prescribing such a toxic and deadly brew?!”
“Calm down,” the pharmacist said, “and let’s see what we can do.”

“Take this to your doctor at home, and tell them this is what Mayo recommends,” I was told by a doctor with an obviously over-inflated sense of self importance, but then who am I to judge. After all, I am the one who sought out the advice of world-renowned experts. “Fine. I can quit those supplements while I’m taking the ARVs,” I told him.
The protocol
Back home, my helpful family doctor is not comfortable prescribing HIV drugs. She knows her place in the system, I guess, and in hindsight, I’m glad I went to see the infectious disease (ID) specialist she referred me to for the drugs instead. Why? Because once the information I am sharing here becomes public, I have serious doubts that the specialist will want to have anything more to do with me, and if I have to choose between two doctors, I much rather have my supportive general practitioner available.
The infectious disease doctor and I both agreed that we can probably cross the raltegravir off the list, and hold it “in reserve”. She is unaware that I have eyes for only two of the drugs on the above list anyway, but it was obvious that she was not going to be receptive to any kind of “thinking outside the box” called The Guidelines. Scheduling appointments and having some required medical records transferred consumed nearly two months after the trip to Mayo. My CD4 counts had continued their steady decline to 97 in April and 70—a new all-time low for me—by May 10. My viral load was bouncing on either side of 1 million.
Finally, with prescriptions in hand; a new Ryan White case manager to synchronize Missouri ADAP (AIDS Drug Assistance Program) with my Medicare drug plan, and Sam’s Club pharmacy, I’m ready to depart on this new journey that started May 23, 2012.

Since I am not taking the Epzicom or raltegravir, I do not fill the prescriptions for those drugs. It’s bad enough that taxpayers are helping to pay the steep price for the drugs I am taking. So far I haven’t been challenged by my doctor, so apparently there is not yet a system for reporting back to her from the pharmacy about what I’m actually having filled.
Notice also that I am taking only half-doses of the darunavir and ritonavir. Just last November, the FDA approved once daily dosing of darunavir at 800 mg, and I knew of those trials when I started my own personal trial. Based on anecdotal reports from sources in Europe, I knew that patients there were having success with “low-dose” darunavir, but I was never able to nail down exactly what that meant.
The only option I had was to make do with what was available to me under the circumstances, and I ultimately opted for the above, half-dose regimen. This decision has required me to do some things I am extremely uncomfortable with, like misleading the doctor who prescribed. I have taken to referring to this as LODOBODAMO (LOw DOse, BOosted DArunavir MOnotherapy).
Results to date
I started taking LODOBODAMO on May 23. Just six weeks later, the viral load had dropped more than 2 logs, from more than 600K to 4,190. Since then VL has dropped to 31 as of December 7, the last time I had labs done.

CD4 counts have been slower to respond than I had hoped, but the decline was halted immediately, and those numbers have been rising, as well, from a low of 70 to 167. Curiously, the red marker, at the bottom of a “dip” after starting the drugs represents a drop of CD4 counts while I was hospitalized with an outbreak of herpes simplex (shingles) in my left eye. Curious, because we’re told that one immune response to such infections is an increase in t-cells, but that’s another mystery to write about another day.

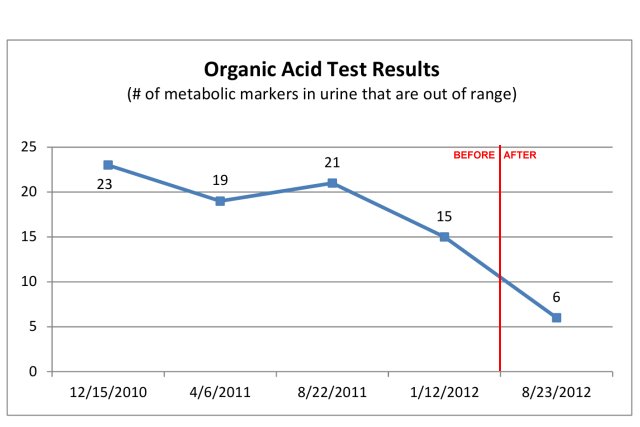
I happen to agree with those skeptics who assert that CD4 and viral load surrogate markers alone are incomplete and inadequate indicators of clinical health, which is why I also have routine blood tests performed, as well as nutritional, inflammation and oxidative redox levels monitored. I will be having some of these tests done again in a few weeks. Meantime, the number of the 72 metabolic markers that are out of range in the organic acid tests (OAT) that I have also been tracking for more than two years dropped by 60%, following initiation of low-dose boosted darunavir monotherapy.
(IMPORTANT UPDATE 2/20/2013: I have updated the information regarding Organic Acid Tests in this post.)
There have been some other changes.
The parotid cyst that defied IVC, UBI and other interventions with natural compounds, has shrunk to almost undetectable size: from a golf ball to a pea.
The other was a setback. In September, I experienced an outbreak of herpes simplex (shingles) in my left eye that was so severe that it required hospitalization and intravenous acyclovir. This was not my first severe outbreak—the first occurred more than three decades ago, long before I was HIV-positive—but it was the first time I’ve ever had shingles inside my eyelids. Hopefully I will write about the possible reasons that incident may have occurred when it did, and yes, it is quite possible that the ARVs played a role, though perhaps in an ironic way.
Visualize
Thanks to a very sociable social networking buddy, John Grosso, I took a break from drafting this post to prepare an online presentation as part of a mutual learning challenge to master the art of “Hanging Out” on Google+ and YouTube (or, as Forbes calls it, GooTube). I’ve taken the liberty of editing the original 97 minute Rainbow Show 1.02 to create the following presentation. Hopefully it will help enhance the information I am trying to share here.
(click link here, if embedded video player does not work)
Where to from here?
As I’ve written about before, there is also some very good evidence—like the LOTTI study—that ARVs need not be taken for life, despite what the pharmaceutical-driven medical system tries to tell us, via The Guidelines. When I re-started the drugs in May, my goal was to be able to quit them before the end of 2012. It is now February, 2013 and I’m still taking them.
This is where I admit that I am at a complete loss about how to make that decision. Frankly, it becomes a psychological mind-fuck. As I state in the video above, the single most significant factor in my decision to re-start ARVs was the sudden—and in my mind, significant—decline in CD4 counts. Had those stayed up, it might have been easier to dismiss the soaring viral load. As it was, the coincidence didn’t allow me to do that. I admit that I want to see higher and more stable CD4 levels.
I have learned before, and am learning again, that it is important to find ways to listen to our own bodies, and mine is telling me it wants to quit the drugs very soon. My intellect is the switchman that is arguing that we wait until we get more information at our mid-month consult at the orthomolecular clinic. One of the things that has always been problematic about my own helter-skelter approach to these experiments is that it is impossible to rule out cumulative, concurrent and even contravening actions on my part. For example, I have not been taking some of the supplements that I think my body probably needs.
It makes sense to me to keep doing what I’ve been doing a few weeks longer and find out what my glutathione, nutritional, metabolic, inflammatory and oxidative redox markers are while I’m taking these drugs. Quitting two weeks before having these tests done seems counterproductive and potentially confusing.
This post has taken more time, energy and effort to construct than any other blog post I have ever written. Just to give you some sense of what I’m trying to tell you, I started drafting it October 19. Part of the reason for procrastinating so long is because I went to ground for the last eight months or so to “work the system”, as it were. Now that I have an 8-month supply of drugs in the fridge, thanks to half-dosing, I don’t really need to play that game any longer. I hope the effort is worth it, because there is still so much to share.
To those of you who have taken the time to contact me, offer encouragement and support, or just to make inquiries or share your own stories; let me say thank you. It helps keep me motivated to know others are out there, to meet some of you, and to share and participate in this adventure I call co-learning.






You are a total inspiration.
Jon:
I have the highest empathy and respect for how you manage your situation, with insufficient reliable mainstream info.
I don’t know what I would do in your situation. However, I have read a lot of the literature, and just the Treatment Guidelines themselves make a very strong case for avoiding ARVs whenever possible. Several posts on my blog have discussed aspects of those Guidelines, most recently “Antiretroviral drugs
lead to normal life?, 2013/01/02, http://wp.me/p8Qhq-xL.
As well as the continuing use of AZT that you point to, I suggest thinking about the fact that the Treatment Guidelines have been modified on an average a couple of times a year, and that once-recommended treatments move to not-recommended. Perusing the Guidelines’ lists of “side” effects is also hair-raising.
For some time now I’ve believed that the greatest gap in our current knowledge is an understanding of the range of significance of CD4 and VL numbers and how an individual might go about finding what they mean in his individual case.
I have always liked your site. 🙂
Jon, I was riveted by your story. This is the first time I’ve heard
anyone else talk about monotherapy and really believed that I was the
only person in the world doing it.
May I just give you a brief résumé
of where I am at the moment? Being an Affected and having started in
’97 on AZT then the usual HAART, I carried on until I realised what it
was doing to me. I stopped taking everything for 6 years, during which
time the “viral load” remained undetectable. It started to climb (I know
why, nothing to do with HIV!) until I had to begin the antivirals
again, but after a year decided that I didn’t want to carry on, and
suggested to my doctor (at a large infectious diseases clinic in Modena,
Italy) if I could just try taking a single antiviral as an experiment.
I
began taking Atazanavir (a protease inhibitor) without booster around
2007 and did just that until June last year (2012) when I stopped taking
it. I remained undetectable for all that time, with no resistance
developed obviously, and as far as I know the last time I went for a
test in July 2012 I was still undetectable, but never even rang to ask.
If there had been any change they would have let me know.
Like you, I
intend starting on glutathione and other supplements at some time, but
at present feel I don’t need to do anything. Listening to your body is a
great feeling, and the feedback is always positive.
I think I was
lucky with my doctor, who is not afraid to try something different but
am sure he gets stick for not being like everybody else. I did ask him
whether anyone else was doing the same as me, and he said I was the only
one. I’m pretty sure though that if I speak with him about continuing
without treatment and maybe taking supplements, he won’t be able to
support me, so that’s why I haven’t been back.
So it was so
heartening to read this. You’ve done amazingly and I’m sure your story
will encourage other people to try. I began to suspect this virus wasn’t
the big baddie everyone made it out to be, and in fact, look how easy
it is to keep it under control! You don’t need big guns to shoot down a
small target, they do more harm than good.
So a huge thank you and keep going and I’ll do the same!
Danny
Hi Jon.
I’m about to stop taking ARV’s for the 2nd time. After stopping the 1st time, I ended up in hospital with PJP (PCP) but I think that my illness was not related to me not taking ARV’s. Nonetheless, it did scare me a bit.
I also feel that if one is wedded to ARV’s, then one is also wedded to surrogate markers. I believe that the psychological connection between these two things is enormous & plays a significant role in whether a person is well, is not well, remains well or becomes sick.
Consequently, I no longer take notice of CD4 counts & VL (viral load) as I believe these markers will do nothing but addle & confuse me. I also believe that these markers are not predictors of anything.
As Mike Hersee suggested, CD4 counts may well be a trailing edge indicator as opposed to being a leading edge indicator.
I’ve had enough of toxic drugs.
I’m fed up with HIV doctors, who blindly quote from biased studies.
I’m incensed at how scientific journals mainly publish “positive” results & hardly any “negative” results.
If all of the above is not enough, I’ve lost friends due to my being labelled HIV positive & I’ve also lost friends who, when I announced that I thought that I wasn’t going to die from AIDS & I was going to stop taking the ARV’s, kicked me out of their home.
The stigma & discrimination is the worst part of this horrible label. Now I know how a lepper must have felt.
All the best Jon. I’ll see you back at QA.
Thank you for posting this… If I have to go on meds it’s good to know there is a low-toxicity mono therapy that’s actually effective.
Hi John (and Danuta, if you’re reading this),
Since you are (or were) on such a low-dose of a single drug, have you noticed any side-effects comparable to when you were on HAART, or any side effects at all? Is there really any health urgency to get them out of your system?
After more than six months on the low-dose darunavir, I did start to experience loose stools and diarrhea. It is eerily reminiscent of the experience I had with HAART more than a decade ago.
While I intend to quit the darunavir, I don’t feel a sense of urgency, in terms of immediacy. I am concerned about potential for long-term adverse effects that may not be recognized for quite awhile.
The trick, for me, is knowing what marker to use at what level, to make the determination to quit. The closest thing I have to a pre-conceived objective or target is probably CD4 >400. and viral load of 4 digits, or less, but I admit that I find those markers to be pretty inadequate.
Thanks, that sounds like a good plan…
I was able to get my viral load down into the 2,000’s a few times from following the alkaline diet, but it was not permanent, nor is the alkaline diet permanently sustainable…
Following the one-dose per day of Prezista and its booster, have you been able to ever get your viral load undetectable or just low down to 31?
When Ruggiero spoke about Prezista did he have anything to say about the booster drug that usually goes along with it? I wonder what the effect of two Prezistas per day without the booster would be?
My viral never dropped to “undetectable”, and that does not bother me.
Ruggiero has never advised me about medical treatment, other than to point out to me the published studies regarding darunavir. I have never seen a study of that drug that did not include using ritonavir (Norvir) as a booster.
I am also curious about what the minimum effective dosing might be, as well as the trade-off between higher doses of darunavir vs. the use of ritonavir, and have even done a bit of self experimentation, which I intend to write about soon.