- Even Dr. Ron seems to be excited about the latest OAT rest results!
The latest round of OAT, stool and conventional “HIV” surrogate test markers are in, and the news is mostly good. Regardless of what angle one looks at these laboratory test results from, there is evidence to support an evolving thesis that a multi-faceted approach to immune dysfunction might be as efficacious as the current pharmaceutical-based guidelines for treating “HIV/AIDS”… minus the worst of the adverse effects.
The not-so-good news is that the continuation of this seven year long experience (experiment?) is being jeopardized by the lack of financial resources. There, I said it, and I won’t mention it again until the end of this post. If you find anything helpful about what I am sharing here, please consider clicking on the GoFundMe link on the right.
Darunavir monotherapy and the orthodox markers
I restarted a reduced dose version of anti-retroviral drugs in May, 2012 after more than ten years of freedom from all AIDS drugs. I had been tracking a long-term decline in CD4 counts to levels I had never seen before: an absolute count of 70 and 7.6%. I wrote about that decision, and about that trend in a post titled “97” which has received more comments than anything else I’ve ever written on this blog. I was overly, some might say desperately optimistic that I would only need to take the drugs for a few months, but I ended up staying on them for a year.
The self-devised half-dose darunavir monotherapy—which I describe here—successfully reversed the decline in CD4 counts, as well as knocked the stuffing out of my sky-high viral load. When my CD4 had risen in May 2013 to 274/13.7%, I quit the drugs again and chose not to re-test these particular markers again until last October. I was indescribably frustrated and disappointed to discover that my CD4 level had dropped to the lowest point ever: 65/4%.
I resumed the half-dose boosted darunavir, and watched as the CD4 jump back up to 180/7.2% by the end of the year, and then dropped a bit to 159/6.9% at the end of January. All of this is charted and can be found under the medical attachments at the top of the page.
What can I say? I am at best conflicted about taking the pharmaceutical ARVs—at any dose. At the same time, I continue to observe evidence of Affected friends who find themselves in hospital emergency rooms and intensive care units with serious and life-threatening infections. Every single one of them to date discovered they had single-digit CD4 counts. Of course some will argue that “correlation does not prove causation,” and I would not disagree. I must, however, respond that ignoring correlation simply because it does not prove causation may prove hazardous to one’s health.
The best I can say is that I am encouraged that these markers are being controlled with a very reduced regimen of antiretroviral drugs, thereby greatly reducing my risk for complications from toxicity and adverse effects.
Healing dysbiosis
What I have been most concerned about and focused on the last two years or so are the dysbiotic markers revealed in bodily fluids other than blood, specifically organic acid tests (OAT) and comprehensive stool analysis (CSA). For three years now the OAT tests have indicated bacterial and fungal overgrowth in the gut, and the stool analyses have more recently confirmed that, as well as provided more specific details and helpful treatment suggestions.
Despite their value and importance, the blood tests that most doctors and patients rely on so heavily have failed to identify these underlying chronic health issues. Even today, there are no significant out-of-range flags on any blood-based tests.
Until recently, my success with controlling the candida and other dysbiotic organisms had been mixed, probably due to my own inability to truly restrict my diet for more than a few weeks at a time. The good news is that my tenacious nature appears to have—so far, at least—won out. It reminds me of my efforts to quit smoking. I failed dozens of times, but eventually I did quit. Here is a very simple graphical overview of three years of OAT results.
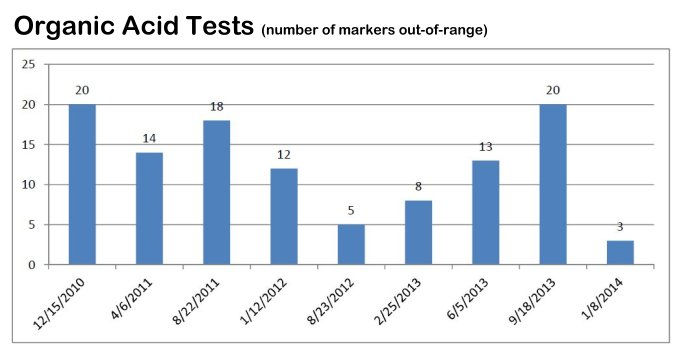
This is a very simplified and non-specific graph, because OAT detects problems other than just gut dysbiosis by measuring metabolites in urine; things like neurotransmitter, bone, fatty acid oxidation, Krebs cycle enzymes and more. Still, it is such an encouraging progress chart. I now have only 3 markers out of range, instead of the dozen or twenty that used to be out of whack. Of those three, one is only moderately out-of-range and another may be elevated as a result of high dose vitamin C. There is a more detailed summary overview of all OAT tests I’ve had done to date here. For those interested in learning more about the kinds of things that can be gleaned from OAT tests (which I highly recommend to anyone with chronic health issues of any kind), read this OAT from December, 2010, as it contains the greatest variety of analyses, one of the strengths of these particular tests. Most “blood work” test results from places like LabCorp or Quest just provide numbers and no contextual analyses, let alone treatment recommendations.
The other test that I started having done in 2012 was comprehensive stool analysis. The first one was done in February of that year by Genova Diagnostics. While that test “suggested some imbalance in bowel ecology”, I have since had these tests done at Great Plains Laboratory (GPL), the same place that does the OAT, as there test provides much greater detail and analyses. For example, GPL not only identified specific dysbiotic bacteria, but also tested for sensitivity to a variety of pharmaceutical and nutraceutical agents.

This has proven to be critical information that I had been lacking! There is all kinds of information online about natural antibiotics and antifungals, but a patient is left with either guessing, or trying to “throw the book” at the gut, hoping something might stick.
The latest CSA came back with no dysbiotic bacteria, though there is still room for improvement in the number of beneficial bacteria, including Escherichia coli. Yes, E. coli, infamously blamed for outbreaks of food poisoning. But only a few strains of E. coli are dangerous and most of them are beneficial and even necessary. Despite this, the FDA has blocked the sale of the only probiotic supplement containing beneficial Escherichia coli. Once again, I find myself considering importing an unapproved product that is legal in Canada and Europe.
The fungus among us
Both the latest OAT and CSA indicate that despite considerable improvement, I have not yet completely controlled the yeast overgrowth.
There is only one yeast/fungal marker that remains out-of-range and that is arabinose, and the level is lower than it has been for more than a year. I have started another round of nutraceutical intervention in an attempt to bring the yeast under control.
Dysbiotic bacteria and yeast can colonize in the gut and form a protective shield around those colonies called a biofilm. Before any antimicrobial—pharmaceutical or natural—can be effective, it must contend with this protective shield. This may well be one of the reasons my initial attempts to control bacterial and fungal overgrowth was not very successful. Last Fall, my orthomolecular doctor recommended I try taking an enzyme-based compound designed to break down biofilm, along with a regimen of natural antimicrobials. I’m convinced this two-step approach worked. I don’t know what else could explain the sudden and remarkable elimination of most dysbiotic bacteria, and reduction in yeast metabolites. The product he prescribed was Interfase Plus. This time around I am trying a product called Biofilm Defense, produced by the same lab that I acquire colostrum from.
Other stuff
In addition to these imbalances in my gut microbiome, there are some other troubling indicators that I am checking into further. Since the first stool analysis two years ago, levels of the digestive enzymes elastase and chymotrypsim produced by the pancreas have been low, and getting lower. The possible causes mentioned include pancreatitis or pancreatic cancer. So far neither of those can be confirmed and I am supplementing with dessicated lamb pancreas before meals. These enzymes are essential for proper digestion of protein.
Lactoferrin levels are high. According to GPL, “Lactoferrin is a quantitative G specific marker of inflammation used to diagnose and differentiate IBD from IBS and to monitor patient inflammation levels during active and remission phases of IBD.” Irritable Bowel Disease. I haven’t really wanted to even think about this until I got the dysbiosis under control, but this marker has continued to rise and is now three times the upper reference range. I will be undergoing a colonoscopy next week.
Then there is the extremely low levels of Secretory IgA (sigA), “which is secreted by mucosal tissue and represents the first line of defense of the GI mucosa and is central to the normal function of the GI tract as an immune barrier. Elevated levels of sigA have been associated with an upregulated immune response.” The recommendations for increasing sigA include supplementing with L-glutamine (which I have done more often than not the last ten years) and to reduce stress.
After the gut, the section of OAT markers most frequently out of whack are those pertaining to neurotransmitters. They are also the most difficult to understand or compensate for, imo. They are the least consistent over a period of time, with different markers veering in- and out-or-range. There was a period of time when none of them were out-of-range, and that period coincides with the time I was taking the darunavir. Only one of these markers was whack at the beginning of this year. This will be worth watching to see what they do in the future. It is not easy to read the analyses for these markers, as they often include words like “Alzheimer’s”, and “AIDS-related dementia”.
Cannabis acupuncture and Chinese herbs
I’ve continued to trial various things to see if they make a difference, either in laboratory markers, or in how I feel. As I mentioned above, one of the recommendations for increasing sigA is to reduce stress. I do practice some techniques, including self-hypnosis and meditation. Something that has always helped, but I can’t self-administer (yet) is acupuncture, and I’m fortunate to know two practitioners I hold in high regard. So I’ve been trying to get at least one treatment a month.
One of these practitioners suggested a formula of Chinese herbs that is popularly prescribed in San Francisco, where he underwent some of his training. I’ve almost exhausted the initial supply, which lasts a couple of months.
Finally, I broke down and ordered some cannabidiol oil from the newly liberated state of Colorado. Cannabidiol is just one of many cannabinoids found in the cannabis plant. This oil contains no THC, the psychoactive ingredient sought by most pot users and for this reason it is legal in all 50 states and can be ordered online. The last thing I need right now is to feel “high”, but I am intrigued by the promising reports of medicinal uses for the plant. I do think that the oil has helped improve my sense of wellbeing and my energy, though that is admittedly a very subjective observation on my part.
But how are you feeling?!
I’ve shared a lot of information here for one sitting, and it started out a mostly a recitation of test results. I’ve said before and I’ll remind myself here that the most important measure of “health” is how I feel. I have to say I feel pretty darned good. I’m not nearly as physically active as I was just a couple of years ago, and I hope that kind of energy isn’t gone forever. I have a home improvement project or two I’d still like to finish.
I don’t know how to assign efficacy or value to some of the protocols I am trying. I do believe the acupuncture helps me reduce stress. I don’t have evidence that either the Chinese herbs or the cannabidiol are “fixing” anything. At the same time I am reminded of the numerous cancer scares I’ve had the last few years, and yet to the best of my knowledge, I remain cancer free. Is it possible that some of these measures have prevented progression to more serious chronic illness? I don’t know, but I can hope.
The fatigue has certainly eased up. I rarely sleep more than six hours at a time, but I almost always sleep at least two shifts a day. Still, it’s probably an average of 8 or 9 hours a day lately. I’ve been working on the new website for a couple of months now. I can only focus on it for an hour or two at a time. Writing a post like this takes several hours over a couple of days.
I see how Michael is slowing down too, and he doesn’t have “HIV/AIDS”. He’s just getting older. It happens, right? That’s a good thing, isn’t it?
Oh, mood, aka depression. I don’t feel any acute depression, and haven’t for some time. I experience the usual niggling anxieties about our future, but who doesn’t? We’ve taken to attending a symphony concert about once a month, and have had visitors and company. The house doesn’t stink; there’s no rotting food in the fridge; the dishes are cleaned at least once a day. We’re diligent about giving our cat Jackson insulin shots twice a day and feed the dogs too.
Boring, yes. Depressing? Nope.
The future
There is one concern I cannot deny or ignore, and that’s financial. I started the GoFundMe campaign about a year ago, and after a brief flurry of contributions, the donations have stopped. The expenses for much of what I’m reporting today have not stopped. I haven’t even updated the expense report that I’ve made public here. Most of these expenses were put on credit cards, so I am also paying interest. Asking for money to help me with my own needs is probably the hardest thing for me to do. The reality is that there is a limit to what I can do. It’s called a credit limit, and I’ve already had that lowered on one credit card.
I would not be in this place today if it were not for friends and strangers who were willing to take a risk. Some of you know who you are. You underwrote the cost of an intravenous vitamin C trial that I wrote about. I still do IVC, but only once a month or so.
You know who you are: the person who has called the Riordan Clinic more than once to make a substantial tax-deductible donation dedicated to my care there. Thank you!
Despite needing to ask for money here, I also give money to causes I believe in. They are always small gestures, but I hope they will be joined by many others and result in a substantial gift for someone in need. It called crowdfunding. No one needs to give a lot, if a lot of people give.
Thanks for considering a donation today, and know that I do understand why some are unable to give right now.
UPDATED:
(Note: I continue to post copies of detailed tests and reports, for those who want to take a closer look. Click the “attachments” tab at the top of the page and select “medical” or “financial”, depending on what you’re interested in seeing.)






Your work on all this is invaluable. You are generous to share it!
Hi Jonathan,
Thanks for all your research and openness. It’s hugely valuable and I wish agencies like the FDA and the CDC could see this and have a reserve fund for such undertakings. Administering it would be problematic, however.
I wish I could donate but I have to be financially very careful at this juncture. If my income picks up, I’ll give.
I’m glad the news is so good and wish you the best going forward.
Best,
John
Hi Jonathan,
Well, I don’t know anything about 99% of the tests you discussed here, but I am intrigued. If they are working for you then I say continue them!
I know you won’t mind me saying this so I hope no one else jumps on me, but I would just caution the start, stop, start of the Darunavir. That may lead to a decrease in efficacy. And you seem to be getting good “markers” that seem to help improve your spirit and a happy spirit is always a good thing.
Keep blogging away and hopefully soon we can do the google hangout we discussed.
Concern noted re: darunavir. There are always risks with self-experimentation. Evidence from the LOTTI study showed that people on continuous ART were more likely to develop “resistance” than those in the intermittent arm. Darunavir was specifically designed to… well, resist resistance.